Someone brought my attention today about the most recent Exley paper out in the press titled “Aluminium in brain tissue in autism” (the title could have been better but well….) and published in the journal “Journal of Trace Elements in Medicine and Biology“.
Let me put this straight, this is not a paper that has evidence of scientific fraud or data manipulation. There is no duplicated images, no suspicious blots. The problem I have with this paper is its deep experimental flaws and data analysis that nonetheless should not have passed through the peer-review filter.
- Before we dive into the paper, lets put the paper into context
Lets just put the paper in the context. It was received on October 26th (Thursday). Came back in its revised form on November 21st on Tuesday and accepted for publication on November 23rd (Thanksgivings for the US, but since the editor-in-chief (EIC) is in Europe no Thanksgiving here). Let that sink it a bit: in a bit more than three weeks, it got send to review, came back from review and got revised in 26 days. In my standard of reviewing for journals and publishing my papers, thats some faster-than-light peer-reviews. I usually wait 4-5 weeks by the time I submit mine and get the editor reply to my submission with the infamous reviewers comments. Does a fast-reviewed manuscript means a bad manuscript? Not necessarily, but it can mean that maybe the peer-reviewed was not optimal, rushed or even worse just botched. Based on the quality of the data presented, I am leaning towards a botched review. Thats quite disappointing because the journal holds a decent impact factor (~3 for 5-year impact factor) and you expect an okay review.
Then comes another problem. Exley published this paper (as well as few others) in the journal…..in which he holds a seat in the editorial board. Nobody can exclude the possible conflict of interest. Consider that: if you were an EIC, would you provide the same rigor and objective decision on a paper submitted by a colleague sitting in your editorial board than a paper submitted by Doe and colleagues?
Not forbidden, but if you can avoid it, avoid it. Transparency is key and publishing in diversified journals (unless it is society-official journals) is an indicator of an healthy research.
Finally, the last thing to keep in mind before I deconstruct the paper is the funding source. According to the acknowledgment section “The research is supported by a grant from the Children’s Medical Safety Research Institute (CMSRI), a not-for-profit research foundation based in Washington DC, USA.” Behind the fancy name is just another anti-vaccine foundation that will play “the vaccine safety” card to peddle their pseudosciences. So we can claim that Exley is a shill for CMSRI, since he received monetary support for his research. Does that mean the research is completely bogus? No, but it means it will require further scrutiny, especially when the claim of the study goes against the consensus in the field (aluminum in vaccines is safe).
Same goes if a study funded by Big Tobacco claimed the absence of correlation between lung cancer and smoking or if Big Sugar claimed the absence of correlation between type 2 diabetes mellitus and consumption of sweetened beverages. - So what is wrong with this paper?
For those who wants to read the paper with me, you can download it here (I assume it is open-access, so you should not have an issue with the paywall). Exley has a publication record on aluminum, especially when it comes to its possible ecotoxicity and the impact of aluminum on certain biological processes.
The introduction is damn short, half a page of a double-spaced document but set the tone, this study will investigate the relationship between autism and aluminum in the brain.
Samples are obtained from the Oxford Brain Bank, but felt short to indicate the source of the tissue (like a catalog number) and how this source of materials was complying with the institutional review boards (IRB). Basically, for any research involving human subjects or human tissues, you have to comply with the IRB that such specimens are used for a certain and defined use and foremost been anonymized.
We have 5 patients that were diagnosed as on the autism spectrum and immediately we can pinpoint an important issue: there are no controls and that’s one of the big and unforgiving flaw of this paper.
The authors then used two techniques to localize and quantify the Al in different cortical regions (and sometimes hippocampal regions). They have used three technical replicates (random sampling from the same cortical lobe) for measuring the Al content using an atomic absorption spectrometry and used lumogallion (aka4-chloro-3-(2,4-dihydroxyphenylazo)-2-hydroxybenzene-1-sulphonic acid, a fluorescent dye initially described to localize Al in plant roots). This dye have an excitation/emission spectra close from FITC/Alexa Fluor 488. It has been also used for live cell imaging , in particular to study how macrophages process Al present in vaccines adjuvants (http://www.sciencedirect.com/science/article/pii/S0022175915001222).
Considering the equipment mentioned in the method, the microscope used provides the right excitation bandwidth filter and provide a long pass emission filter for anything over 510nm.Then things get weird, in the result sections, the authors mention the following:”We examined serial brain sections from 10 individuals (3 females and 7 males) who died with a diagnosis of ASD and recorded the presence of aluminium in these tissues (Table S1).“Where is the number coming from? Why don’t we have the same numbers in the Materials and methods?The other problem is the over interpretation of the data. To be brief, the lumogallion will show some punctuated pictures. The authors show some brightfield pictures overlapping to show the tissue structure but does not really help the reader. A DAPI stain (to stain cell nuclei) as counterstain would have been much more informative, it would helped to distinguish background noise from possible Al inclusion. Again, keep in mind we have no controls. The other issues with immunostaining is the high risk to cherry pick the data. You will be naturally inclined to show the presence of a positive risk but this cannot be used for quantitation. Thus, the use of the second method is welcomed as a complementary technique.
For those not familiar with fluorescence, there is an important notion to keep in mind when analyzing the data: ensuring you keep the same exposure time, the same brightness or contrast and foremost have a negative control to set your exposure time. You can see a sketch explaining here on one of my fluorescence staining (based on my data, I concluded the expression was weak if not negative).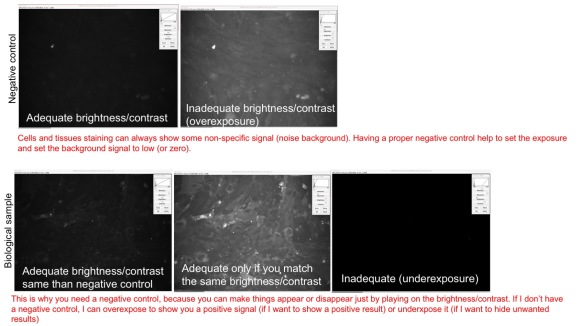
The background subtraction is also a bit weird. I acknowledge the assessment of autofluorescence is a good control, but you expect to see a low staining. But foremost, you cannot overlap two distinct slices, as proximal as it can be. For instance, in Figure 1, you see some lumogallion staining and below the fluorescence from the “control” using the adjacent slice. The lumogallion also seems to have a very high background.
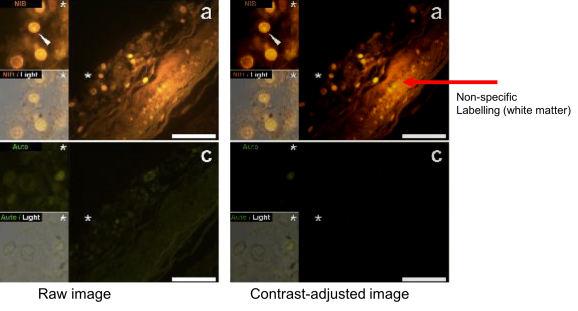
It seems lipid-rich environment increase dramatically the fluorescence of lumogallion (if you look at the spectra, the dissolution of the dye in Triton-X100 solution (b, a detergent) dramatically increase the excitation and emission spectra compared to water (a)).
What I found troubling is this sentence in the results section: “We examined serial brain sections from 10 individuals (3 females and 7 males) who died with a diagnosis of ASD and recorded the presence of aluminium in these tissues (Table S1). Excitation of the complex of aluminium and lumogallion emits characteristic orange fluorescence that appears increasingly bright yellow at higher fluorescence intensities. Aluminium, identified as lumogallion-reactive deposits, was recorded in at least one tissue in all 10 individuals. Autofluorescence of immediately adjacent serial sections confirmed“.
If you are a bit a fluorescence microscopy savvy, you know that the “emission color” we see in the objective is never caught by the CCD camera. These camera have in the most majority a B&W output for the simple reason that they have a much higher sensitivity than color cameras. You can always re-create colors in the micrograph pictures using various “lookup tables” (LUTs) that will give a pseudo color based on the level of grays. This is very useful when you samples different excitation/emission channels (for instance, samples stained with DAPI and two antibodies, one conjugated with Alexa Fluor 488 and the other with Alexa Fluor 546 or further down).
The problem inherent with fluorescence is you can make thing fluoresce or end up with a false-positive signal if you increase the light beam (usually never happens because it is set) or if you increase the exposure time of your camera (this is the most common issue). As you increase exposure, you increase the risk to capture non-specific signal like autofluorescence signals.
The other problem here is how to explain this sudden shift from orange to yellow? This seems more like a subjective observation than something caught on camera. That can be due to different things. You can have some bleed-through of the dye that is normally emitting in a certain wavelength but if it is strong enough can appears in neighboring emission channels. This thing rarely happens with a good fluorescence microscope that have defined filter cubes that allows the diffusion of certain emission wavelengths (for instance, my microscope have a DAPI, Alexa Fluor 488 and Alexa Fluor 555 cubes that only let the respective emission wavelengths with 20nm-margin error to cross through the objective and reach the camera and binocular).
Usually, we have to deal with bleed-through when you use flow cytometry and usually is solved using fluorescent dyes latex beads and by following a protocol called “compensation” (this has the result of removing any noise and keeping only the signals).
We cannot also exclude that such fluorescence is just an autofluorescence from lipofuscine inclusion bodies. Lipofuscin is a lipid-based compound naturally produced by our cells. It has an important concentration in the central nervous system, however it is normally cleared out by cells. Failure in the clearance of lipofuscin is associated with different diseases called “lipofucsinosis” such as Batten’s disease. Even the author admit the possible presence of lipofuscin inclusions “Intracellular aluminium was identified in likely neurones and glia-like cells and often in the vicinity of or colocalised with lipofuscin (Fig. 5).” Lipofuscin is also capable of autofluorescence, although it is more in the wavelengths matching DAPI. Lipofuscin has an excitation/emission peaks at 360 and 435nm respectively but has been reported to also show fluorescence at 510nm when excited at 488nm (https://www.sciencedirect.com/topics/neuroscience/lipofuscin).
Compared to the lumogallion excitation/emission spectra (507/567), we cannot exclude the presence of a phenomenon called “FRET” (Fosterman Resonance Energy Transfer) in which the excitation of lipofuscin (as the microscope excitation bandwidth is 470-495nm) provide enough energy to the photons emitted by the lipofucsin to excite nearby lumogallion dyes. Because the microscope setting used in this paper has no restricted bandwidth (it let pass any photons harboring a wavelength of 510nm and more), it may explain this orange-to-yellow transition noted by the author. The presence of a DAPI nuclear stain would greatly helped to identify this region as grey matter (rich in cells) or white matter (rich in lipid-rich myelin sheets). Thus, we can legitimately questions the nature of these as it these punctae labelled as “Al inclusion” are simply lipid inclusion or some artificial noise due to the tissue processing. This is where controls come as critical, it can help you sort the signal from the noise.The second big issue with this paper is the over-interpretation of what the experimenter see. The experimenter wants to see Al inclusion in monocytes? So be it: “Aluminium-loaded mononuclear white blood cells, probably lymphocytes, were identified in the meninges and possibly in the process of entering brain tissue from the lymphatic system“. Or maybe these are astrocytes, or neurons, or microglial cells, or blood vessels….or whatever the author wants to believe in: “Aluminium could be clearly seen inside cells as either discrete punctate deposits or as bright yellow fluorescence. Aluminium was located in inflammatory cells associated with the vasculature (Fig. 2). In one case what looks like an aluminium-loaded lymphocyte or monocyte was noted within a blood vessel lumen surrounded by red blood cells while another probable lymphocyte showing intense yellow fluorescence was noted in the adventitia (Fig. 2b). Glial cells including microglia-like cells that showed positive aluminium fluorescence were often observed in brain tissue in the vicinity of aluminium-stained extracellular deposits (Figs. 3&4). Discrete deposits of aluminium approximately 1m in diameter were clearly visible in both round and amoeboid glial cell bodies (e.g. Fig. 3b). Intracellular aluminium was identified in likely neurones and glia-like cells and often in the vicinity of or colocalised with lipofuscin (Fig. 5). Aluminium-selective fluorescence microscopy was successful in identifying aluminium in extracellular and intracellular locations in neurones and non-neuronal cells and across all brain tissues studied (Figs.1-5). The method only identifies aluminium as evidenced by large areas of brain tissue without any characteristic aluminium-positive fluorescence (Fig. S1).”
This is the second big mistake of this paper. If the author wants to make the claim he proposed here, then he has the obligation to show a counterstain using selective markers for neurons (e.g. MAP2, bIII-tubulin, NeuN….), astrocytes (e.g. GFAP), microglial cells (CD11b), leukocytes (CD3), macrophages (CD45), blood vessels (e.g. PECAM-1, claudin-5). This could have been easily performed (using a secondary antibody conjugated with Alexa Fluor 555 or better Alexa Fluor 647) and would have give support to this claim.
If the author can identify cells by the naked eye, he is either equipped with Superman X-ray eyes or he is just imagining things.The discussion quickly gets into an anti-vaxxer diatribe and throws the minimal amount of scientific data under the bus.
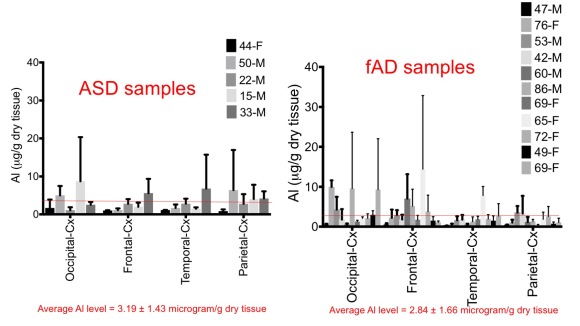
For example, the author throws this sentence as is: “We recorded some of the highest values for brain aluminium content ever measured in healthy or diseased tissues in these male ASD donors including values of 17.10, 18.57 and 22.11 g/g dry wt. (Table 1).” Firstly, where does it get this data? You cannot sum technical replicates, you have to average them (even with considering the huge variability between technical replicates). Secondly, how can the author make a claim like this without providing values from controls (well there are no controls) or from the literature. It is like “we have recorded the highest amount of leukocytes in ASD patients blood samples with values of 11.3, 12.0 and 11.5 x10e3 cells/mm3.” I cannot make an interpretation or conclusion without knowing the reference from the normal population (normal range 4.5-11x 10e3 cells/mm3) or from control groups. The average Al level was 2.38-4.79 microg/g tissues in male ASD and 1.15 in the female ASD patient. Such levels were very similar to those reported in samples from patients suffering from familial form of Alzheimer’s disease.
The data is interesting but we are lacking additional female samples to make a claim as he did: “All 4 male donors had significantly higher concentrations of brain aluminium than the single female donor.” He lacks the proper conditions to run the statistics (you need same number of patients in male and female to make such claims) and even the important inter-individual variability makes it unlikely that he could achieve the statistical significance. This is a statement that would put a graduate student in shame for overconfidence in the data.
Then goes the tirade “What discriminates these data from other analyses of brain aluminium in other diseases is the age of the ASD donors. Why, for example would a 15 year old boy have such a high content of aluminium in their brain tissues? There are no comparative data in the scientific literature, the closest being similarly high data for a 42 year old male with familial Alzheimer’s disease (fAD) [19].” (another Exley paper published…..in the same journal). We are dealing with the same issues (lack of controls, huge variability in the technical replicates…..).
Now if you plot the average patient Al levels agains the age, regardless of the condition, you end up with an homogenous cloud. Now, two things have to be noted here: seems there is no impact of Al levels based on the disease (only age seems to matter between ASD and AD) and there is no correlation between increase in brain Al and age, at least in the very small sample size.
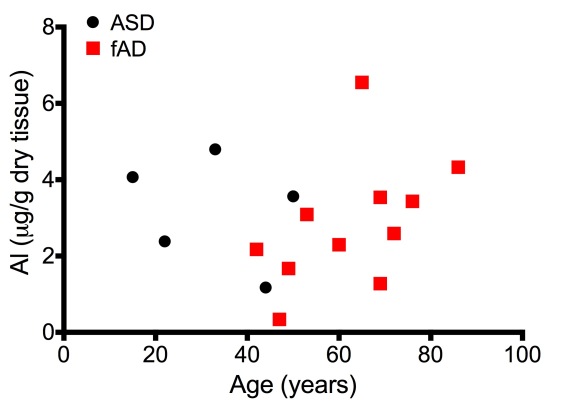
No pun intended, but the data scatter looks vaguely like the United States map. Again, it shows the need of data from asymptomatic patients to estimate the burden of Al in the brain.
Since we have not access to Al content in the brain, we have to see some values in the literature. A study by Andrasi and colleagues (https://content.iospress.com/articles/journal-of-alzheimers-disease/jad00432) provide some Al levels in control samples. According to their study, the average Al content in control samples were between 1.4 to 2.5µg/g dry tissue. We are indeed not far from the value reported by this study, especially when you consider the important standard deviation in these samples.Maybe it is also to consider the other study by Exler on Al level in brain samples from patients associated with familial form of Alzheimers disease (fAD) and familial dementia. In that study, all reported with Alzheimers (some with early onset, some with late onset based on age), the Al values reported were ranging from 0.34microg/g tissue (male) to 6.55microg/g (female, presenting a mutation in the PSEN1 gene, a known gene in FAD). So are we just measuring noise and try to extrapolate data from noise? Thats some bold statement that should have been smashed already by a decent reviewer in the field of neurosciences.
But seeing these two papers went through in a apparent free ride is not looking good for the journal integrity. - Conclusive Remarks
To make a claim is one thing, to back it up with robust data is another thing. I think Exley jumped the shark a while ago and started to aluminum as the big bad wolf in every little things. But a wolf can be tamed, kept out from showing danger to the community and somehow co-exist. But for Exley, like Shaw, like Gherardi, aluminum is the devil incarnate. God forbid it has been used for 70 years and showed barely more than simple coincidence in its association with some disease, aluminum is their dead horse that worth being beaten again and again. If your funding sponsor will give you money for showing a link between aluminum and autism, lets give them what they want. Ethically it is insane, but when you need to keep your lab and your faculty position afloat, sometimes making the pact with the devil and throwing the scientific integrity and the philosophism that is given to you following your thesis defense can be tempting. Sometimes, it feels that anti-vaccines researchers are like Faust and succumbed to the offer made by Mephistopheles offer. But this come with a price and a hefty price to pay: the loss of your integrity as a scientist.
So my question is what is coming next to patients on the spectrum: does this study will be used to support the anti-vaccine agenda (another reason to yell “Aluminum is a chemikillz” in parenting groups?) and breakdown the herd immunity? Bogus remedies by bleach enemas and drops (the infamous CD/MMS)? or give a support to chelation therapy? gluten-free/casein-free diet? Or like Exley once claimed have these people drink ad nauseam silicon-rich water like Fiji water or Volvic water with the magic claims that the silicon with drain your brain from the Al contained inside it?
This kind of deeply-flawed studies, lacking proper controls and driven by an ideology over the facts are dangerous because they prey on the meek and enrich modern snake oil sellers.

{kind=link}
31 replies on “[Neurosciences/Aluminum] Does the latest paper from Exley show a link between ASD and aluminum?”
[…] to the fluorescence microscopy, The Blood-Brain Barrier Scientist knows a lot more than I do, and blogged about this study. This analysis is a lot more technical than mine, particularly for the fluorescence microcopy. The […]
LikeLike
Response by Prof Dave Hoole, head of Prof Exley’s faculty at Keele:
“I am, of course, aware of Professor’s Exley’s research work and his extensive investigations of the possible effects of aluminium on tissues. The goal of any scientific study is to propose ideas that either support or reject hypotheses that are open to test and trial by ones peers and society in general. Only by such debate and testing are advances made. Inevitability this can lead to controversy. Professor Exley has received funding from a wide range of funding bodies and applications are peer-reviewed. In addition, most publications in science which appear in learned journal are peer reviewed before being published. This has happened with many of Prof Exley’s publications.
“All Universities stimulate debate in their search for truth. By such a mechanism significant advances are made. Like you, as is the case with all scientific study, I await to see if eventually Professor’s Exley’s hypotheses are accepted or rejected.”
LikeLiked by 1 person
Thank you for your reply. Since I cannot provide a direct reply to Pr. Hoole, I will use this one as an official reply:
Dear Prs. Hoole and Exley,
I would like to thank you for providing your comments and feedback on my blog post. It is not everyday that as peers we openly provide our comments on a broad daylight.
As a mentor, as a colleague I am calling you to carefully reconsider the utmost principles we all agreed when we have defended our doctoral thesis: we accepted the title of Ph.D. by our examiners and became their peers by showing them our understanding of the scientific process and developed a critical thinking during all these years spent on the lab bench, these hours spent in the lab at night and in the weekend. All of us were driven by one goal: prove or disprove our main hypothesis of the research project we were assigned.
A tenet of testing an hypothesis is to follow the scientific method, following the foot steps of Claude Bernard.
To validate or invalidate an hypothesis, we learnt the utmost importance of having controls. There is no negotiations, no discussions of the needs of controls in each of our experiments. They are crucial to sort fluctuations and errors inherent to the experimental paradigm from the real outcome induced by a stimulus or by a disease condition. This concept is probably the first concept we learnt as graduate students. We always ask our mentee to show us the controls before making a conclusion about the data. We, as peer-reviewed, expect and require any manuscripts to show us control conditions to assess if the conclusions and claims are valid or not.
Yet, the most recent publications by Pr. Exley published in the journal “Journal of Trace Elements in Medicine and Biology” are worrisome. Not because they provide an interesting paradigm that worth further investigation and independent reports by other research groups, but because it displayed major methodological flaws that should not have been resulted in their publications. These are my major comments and point of concern as a peer-reviewer:
1) The foremost major issue is the lack of controls. In that particular case, the absence of samples obtained from patients that did not display signs of ASD or other neurological disorders. This is an important criteria that is essential for any scientific study. For instance, how can we interpret a blood glucose level of 3g/L in patients without knowing the average level found in healthy individual (hint: the average is 1g/L in the healthy population, thus we can conclude that such patients are undergoing a severe hyperglycemia and if left untreated are at risk of dying of diabetic ketoacidosis).
Without controls, we cannot conclude how high the aluminum in the ASD brain samples are.
2) We have a consistent outlier technical replicate in both of the studies. These are inherent to the methodology (three replicates) and the detection method. I would have requested that Pr. Exley try to increase the number of replicates to four for each patients to have a better data scatter.
3. The issue with the use of the lumogallion in this experimental setting is the close proximity in terms of excitation/emission spectra of lipofuscin. We cannot exclude some bleed through and FRET phenomenon that can lead to a false positive. In particular, the absence of filter cubes that can restrict the emitted light into particular spectral bands, in particular for the lumogallion. Sidenote, the description of a shift of orange to yellow tones by increasing sample illumination is irrelevant for the CCD camera (because a decent CCD camera is a B&W camera) but raise the issue of non-specific fluorescence.
4. The description of cellular structure by Pr. Exley in his manuscript is, for a trained microscopist, disturbing. The author describe the presence of Al particles (as labelled by the lumogallion) in various cell types and in various tissular compartments without providing any evidence of his claim. He claims the ability to observe nuclei structures “Cells that morphologically appeared non-neuronal and heavily
loaded with aluminium were identified associated with the meninges (Fig. 1), the vasculature (Fig. 2) and within grey and white matter (Figs. 3-5). Some of these cells appeared to be glial (probably astrocytic) whilst others had elongated nuclei giving the appearance of microglia”.
Such statements are ludicrous and worrisome coming from an established researcher. First, you cannot observe cell nuclei under the fluorescence microscope without a nuclear counterstaining (DAPI). Second, you cannot identify cell types in a tissue solely on a phase contrast. To support such claims, you have to provide a cell-specific marker for each cell types (e.g. GFAP for astrocytes, CD11b for microglial cells….). Thirdly, you cannot at this resolution and this kind of microscopy provide any information on the cellular localization. You may distinguish presence of perinuclear or intranuclear particles (if you provide a DAPI staining), but you cannot claim you can sort intracellular from extracellular content without providing a counterstain (e.g. F-Actin or tubular counterstain).
As I said, the results from Pr. Exley are interesting but in my opinion are too premature and should not have been accepted as is without a major revision to address the experimental flaws. Considering that these two papers were published in a journal in which Pr. Exley sit in the editorial board, we can rightfully raise the presence of a possible conflict of interest and question the objectivity of the EIC to weigh on the final decision made for the acceptance of the journal. Providing the reviewers comments public would help discard this claim and bring transparency on the publication process.
We may argue that such study may have little impact and only constitute an single study that needs to be further investigated. However, we are living in an age of information spreading as fast as light and maybe amplified from an anecdotal observation into an irrefutable proof by individual lacking the concept of science and critical thinking. For instance, JB Handley, an individual known for his anti-vaccine stance, did not wait to propel this study into mainstream news (via Medium) as an irrefutable evidence that Al in vaccines cause autism. (https://medium.com/@jbhandley/new-study-massive-aluminum-levels-in-autism-brains-is-this-the-smoking-gun-for-vaccines-54ae85ec2a9c). Although the link between autism and vaccines have been refuted over and over, anti-vaccines groups (including the funding agency that funded this study) are maintaining their goalpost moving tactics to keep demonizing vaccines. Yesterday it was thiomersal, today it is the aluminum, tomorrow it will be the saline solutions used to reconstitute these vaccines as culprit.
The science is clear, vaccines benefits to prevent infectious diseases hugely outweighs the possible risks associated with vaccines. The odds of developing an serious adverse reaction to vaccines are smaller than being bitten by a shark or struck by thunder.
Autism Spectrum Disorder remains foremost a condition driven by genetic risk factors, with evidence of maternal infections during pregnancy as an other risk factor (thus the benefit of vaccines to prevent such events to occurs).
By having an unnecessary and unjustified media amplification, this study is contributing in instilling fear in parents and pushing modern snake-oil sellers to propose dubious or banned “therapies” including the use of chelating agents, chlorine dioxide (bleach enema known as the MMS/CD protocol), restrictive diets (casein-free/gluten-free diet) or non-approved FDA treatments such as stem cells or GcMAF in rogue clinics to young patients on the spectrum.
If we want to sort out the contribution of Al in ASD, let’s do it by providing a robust experimental paradigm with appropriate controls, lets ensure we have a mutual expertise to ensure the production of data with the utmost quality and accuracy.
I would be more than happy as a peer to help you contribute in such aspect by providing my expertise in the blood-brain barrier field.
Respectively yours,
The blood-brain barrier scientist.
LikeLike
“Although the link between autism and vaccines have been refuted over and over, anti-vaccines groups (including the funding agency that funded this study) are maintaining their goalpost moving tactics to keep demonizing vaccines. Yesterday it was thiomersal, today it is the aluminum,”
The only vaccine that has been studied in relation to autism is MMR. And it does not contain aluminum.
You cannot use studies of thimerosal to support claims about the safety of Al adjuvant. Thats clearly not logical or rational.
Moving interest from thimerosal to aluminum adjuvant is not moving goalposts. It is a change of hypothesis in response to changes in the scientific evidence. This is the scientific method, properly applied.
Moving goalposts is changing targets or thresholds previously declared to provide or disprove a hypothesis. Here is a definition:
“Logical fallacy. Moving the goalposts is an informal fallacy in which evidence presented in response to a specific claim is dismissed and some other (often greater) evidence is demanded.”
Clearly this does not apply to thimerosal and aluminum adjuvant. They are completely different hypotheses, not the same hypotheses with different standards of evidence.
ScientistAbe-are you going to respond to my rebuttal of your fatally flawed and profoundly misinformed article about Al adjuvant transport and kinetics?
LikeLiked by 1 person
[…] in town.”) An actual scientist who does the sort of fluorescence microscopy that Exley found his methods to be…lacking…as well, as did our feathery friend The Skeptical Raptor. Not surprisingly, the antivaccine […]
LikeLike
You almost had me until the end there when you basically had nothing to remark aside from the same old media, brain-washed diatribe we’ve all heard a million times before: “it’s not aluminum,” “vaccines are safe & effective,” “the only valid science is pro-vaccine [pseudo] science.”
Blah, Blah, Blah.
Riddle-me-this Mr. Brainwashed Science Man:
If Vaccines are SO SAFE and SO EFFECTIVE then why won’t the CDC (or whoever else YOU would trust) do a vaccinated vs unvaccinated, double-blind placebo-based study??
That’s all they have to do to shut us up! It would be so simple, but they refuse to do it. Congress refuses to subpoena Thompson over his allegations of fraud at the CDC. Why?
Sorry, bro, but you cannot consider yourself a true scientist if you can’t be just as critical of the studies exonerating vaccines.
LikeLike
Hi Brie, thanks for your note. I don’t think you came by pure randomness but maybe just to troll a bit don’t you? Come on, lets have a discussion between adults and answer your riddle.
You know why we don’t do vaccinated versus non-vaccinated? Because it is unethical. Can you imagine injecting a saline solution to patients and tell them “you should be protected against infectious disease X”. Thats completely unethical and will not fly in an IRB protocol. We do RCT double-blind studies on patients that have already a condition, usually a small population (in Phase 2 trial) and we inform their ability to drop whenever they feel a concern. Double-blind studies are usually kept but when there is a great benefit noted (for instance a drug candidate stop the progression of an incurable disease) then we lift the double-blind and allow every patients to benefit for the treatment.
Now if Big Pharma was so evil and that the health organizations were in the pocket, you would not see what is currently happening for the Dengue Vaccine. Sanofi published a study showing that his vaccine against Dengue can induce complications in naive patients, whereas it showed some protection in those already infected by this virus. Dengue fever is a nasty condition affecting population in developing countries.
If I was Big Pharma, I would hide this study under the rug and keep selling vaccines as usual.
If you really want to do some research and see how I conduct research, my lab is always welcome to those who wants to learn.
Cheers,
Mr. Brainwashed Science Man.
LikeLike
Hi BBB Scientist,
Thank you for your post.
It is understandable that doing a vaccinated vs unvaccinated study is unethical. However, would it be possible to do a study between vaccinated with aluminium adjuvants vs vaccinated with other adjuvants? I see in the CDC webpage (https://www.cdc.gov/vaccinesafety/concerns/adjuvants.html) that there are other adjuvants used so I was wondering why not do a study of that sort if possible. I guess this might not be your field of expertise but perhaps you can shed some light on my question.
LikeLiked by 1 person
Hi Diego,
Thank you very much for your email. I try to do my best to give you an answer, because as you mentioned it is beyond my expertise.
For the aluminum adjuvant, historically it was done by Joseph Bell in his two publications in JAMA in 1948 (pertussis vaccine and diphtheria vaccine) in which he took the same vaccine lot (without adjuvants), randomized patients into two groups: one received the vaccine as-is, the other one the vaccine supplemented with alum. He followed up the cohort in a double-blind study for 2 years and concluded that the group recieving the one supplemented with alum adjuvants fared much better.
Once you have evidence that an adjuvant or a change in the formulation result in a better immunity, it would be in my opinion pretty unethical to revert into a formulation that gives you less protection.
Now, there are a new generation of vaccines candidates coming out for COVID19 which are likely having an arm (or group) with a saline preparation versus a formulation considered optimal, as new as new adjuvants. I would say it would be interesting to follow these up, because maybe there maybe new adjuvants that maybe tried for COVID19 and possibly investigated later against aluminum-based adjuvants.
I think there is a need for a new generation of adjuvants as there are still some vaccines that can do better in terms of efficacy (I am thinking about the DTaP which require regular boosters).
I would say the identification of new adjuvants will be made possible as we better understand immunology (I call immunology the quantum physics of biology. Every time I think I understand it, changes in the field put me all upside-down).
LikeLike
Thank you for your reply Scientistabe!
As you said above, research methods have changed a lot through the years making a lot of studies obsolete, so perhaps it is time to revisit studies that are so relevant for today’s decisions and yet were done such a long time ago.
I definitely hope all this research into the covid-19 vaccine brings advancements in the field of immunology, as there are tonnes of bright possibilities for non-infectious diseases.
You see one thing I think its important that doctors and researches keep in mind, is that a lot of parents like myself worry more about the diseases that we have no clue about their origin and don’t have a treatment (or its not easy) and that are on the rise, like authism, cancer, etc. I read that about 1 in 50 kids born in the US will have authism, tell me that doesn’t scare you. So its tough facing the decision to give preventive treatment to your kid when you realize some components are actually toxic. Anyhow just wanted to give you a thought into what I think drives all the questioning of the standard practices, especially given its common to see bans on substances that were once thought to be safe.
Thanks again!
Best regards,
Diego
LikeLike
In the 30ies of the last century many studie were performed to validate efficacy and safety of Diphtheria vaccines.
The outcome was, that some vaccines did not work, but some did.
From those who did work further diphtherie vaccines were developed.
E. L. Bauer in Philadelphia between 1925-1930. vaccinated people 960252 from this group 21 got diphtheria, compared to 104732 of unvaccinated people 4891 got the disease ( Risk ratio vaccinated /unvaccinated 1:230 .
I think this high number of people included should convince people that more studies are not necessary (but had been performed in 80-90 yrs ago.
So the claim of testing vaccinated versus unvaccinated is ridiculous. This was done 90yrs ago- but is not in the www. The data are not so easy to find.( ED Bauer A survey of diphtheria prevention in Philadelphia Amer J med Sci 182: 839ff (1931). But the data are available online.
Just look at it.
LikeLike
Hi Wolfgang, thank you for your comment. The article maybe interesting but it has two major caveats that needs to be adressed:
1. It is a very old paper (1931). What was probably true back then maybe not, because we have improved the scientific methods, have better tools to analyze the outcomes. To give you an idea, we consider scientific papers obsolete within 10 years after publication, as science move and analytical methods are refined.
This paper maybe worth for its historical purposes but it may have little or no relevance nowadays. I can cite papers in the BBB field before the groundwork of Reese and Karnovsky, some of them were suggesting that the blood-brain barrier was just an technical issue due to dyes charges. That of course got refuted by the late 60s.
2. It is important to see how it fared to the existing literature back in the days. For an historic standpoint it is interesting, remember this is a time in which Pubmed was not existent yet and the spread of information was very limited. If you type “diphtheria prevention” in Pubmed and got to the last pages, you can find several pages with archived PMC articles scanned from these archives that can give us an overview of the situation. This is important because it helps to place this paper in the context and how it fared to other reports. You have to put this back to the first report of Ramon of the diphtheria anatoxin in 1924, so we are within less than 10 years since the first report by Ramon. There is this study in 1930 from Ontario that show the drop in the number of diphtheria cases and deaths associated with following the introduction of the anatoxin. By its own, it is almost a multgicentric report and showed a decrease in years following the toxoid introduction.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC381997/?page=1
LikeLike
I only mentioned this studies, because many “critcal” people complain about the fact, that in nowadays clinical trials, they have never been real placebo double blind controls. Meaning that a vaccine (Antigen + adjuvans) was tested against adjuvans. Today such double blind studies are considered unethically, but such studies have been performed 100 yrs ago.
In rare cases one will find vaccinated versus unvaccinated children – I am aware of one (small) study from Nigeria Epoke J et al Vaccinated versus unvaccinated children; how they fare in firstnfive years of life Trop. Geog. Med 1990;42(2) 182-4
LikeLiked by 2 people
Thanks Wolfgang for your input. Your point is relevant because the placebo (saline with adjuvants) versus treatment was considered okay before 1945. If we think about it, the “clinical trial” of Louis Pasteur on Joseph Meister by inoculating it with a attenuated strain of the rhabdovirus (rabies) would have made never get an IRB at first, not even an IND classification by the FDA. Then came the atrocities of the Nazi scientists in the concentration camps (I come from a French town that has been annexed by Nazis and had the school of medicine headed by Nazi physicians) followed by the trial of these physicians in Nuremberg in 1946 (this one is less known by the public, as the main trial usually eclipsed it) that set the groundwork for bioethics and patient consent in clinical trials.
Interesting paper, unfortunately the journal died a long time ago and it seems getting the hand of a hardcopy will be a quest. But from reading the abstract, we can suspect that the control group was involuntary group in the sense that they were not refused access to vaccines. They were just not vaccinated or did not have access to immunization campaign (as my understanding) and they mostly maintained a five-year records on 25 children from their birth until their five-years birthday. It is important to note that out of the 25 vaccinated, none of them died and one got an episode of measles (mild form). The unvaccinated group reported three fatalities (2 from measles, 1 from tetanus) and 11 got infected from a measles outbreak in 1986. It shows the importance of vaccines and wide-spread immunization, in the bright side the access to immunization is cheaper than ever and now should cover these communities that were out of reach 30 years ago.
LikeLike
Nobody disputes the effectiveness of diptheria vaccine.
The primary concern and argument of vaccine critics is that vaccines are not safe. That they cause long term neurological and immune system harm. Today, strong evidence implicates the aluminum adjuvant (or other adjuvants) as the cause of the problem.
Did the study you cite attempt to determine long term or neurological or immune system outcomes from the vaccine? I have seen many old studies supposedly showing vaccines to be safe, but they always fail to look for such outcomes. The follow-up periods are too short (few days or couple weeks), and they dont look for neuro or immune-related health outcomes. As evidence for safety, they are garbage.
LikeLiked by 1 person
From a practical point of view a placebo controlled double blind study in adjuvanted vaccines is not possible. If one arm would be the antigen + Al-adjuvant (this is a milky suspension) and the control arm would be saline (this is a clear solution) , one would see immediately what is the verum and what the placebo- that is not double blind. With non-Al- adjuvanted vaccines like Influenza vaccines this would be easy, and has been done. In addition a saline placebo would have a higly different viscosity, compared to the verum. So a second chance would exist to differentiate the verum from a placebo. One would feel the different pressure during injection.
But until know a safe substance with a milky impression, but not containing Al-adjuvans was not found.
LikeLike
In study, I looked at plant life uptake of aluminium, and how plant deals with al toxicity by forming a node, isolating the toxin from the higher reaches, branches, leaf. Etc.
It can cause localised dieback of tissue,, as the narrowing of the plants transmission paths encourages blockage. The electrical nature of the brain attracting metals exacerbating the problem, especially in the high neural impulse areas around memory function, encourages concurrence with the original papers finding, as by different paths, we have arrived at the same conclusion. I had no initial Bias either way, but deduction leads in precisely the same direction.
LikeLiked by 2 people
Hi J., thanks for your comment. The problem is you cannot translate what happens to plant into animals, even less to a mammalian brain. The electrochemical nature of the brain is tightly regulated, it is not as we may conceive a free circuit. Why? Because of myelin sheets present in the oligodendrocytes wrapping axons in the CNS, Schwann cells in the PNS. You only have very tiny openings called Ranvier nodes that works by allowing the only exit/entry of ions to propagate the electrical current within the axon. In addition, you have the BBB that would add an additional layer. If your hypothesis would be correct, then molecules charged or not would free flow into the brain. Thing is that charged molecules cannot cross the BBB unless they have a solute carrier.
Aside of Neurosciences 101, you also agree that making a claim without having proper controls (negative and positive), you cannot make a claim. That’s something on this paper was clearly missing.
LikeLiked by 1 person
@J Frodsham,
In plants something is different. Many plants have defensive forces (in acidic soil) to avoid intoxication from (soluble) Al3+.
But horsetail plants – which belong to the oldest plants during evolution- do life with Aluminium- for them Aluminium is an essential element, they need it.
And other plants accumulate Al – such as tea plants- some plants are even hyperaccumulators – these acculumlate Al in their leaves.
LikeLiked by 2 people
[…] Does the latest paper from Exley show a link between ASD and aluminum? […]
LikeLiked by 2 people
[…] more about his misleading “study” & why it’s a great example of bad science here & here & here and […]
LikeLiked by 2 people
[…] Does the latest paper from Exley show a link between ASD and aluminum? […]
LikeLiked by 1 person
I don’t trust you. You are clearly biased in favour of mainstream narratives. You would quite happily have millions of people take risks instead of being reasonably cautious. You are the proverbial tail wagging the dog. ‘Instead of being cautious, we’ll use these chemicals all over the place until it’s proven that they’re safe. Because we are establishment scientists and we know what’s best.’
Accuse me of being a troll. But I don’t trust you. I think you’re a slavish adherent to establishment dogma. You may as well wear a dog collar and give sermons once a week.
LikeLiked by 1 person
Hi Simon,
Thanks for your comment. You see I don’t ask people to trust me and I always welcome constructive criticisms and fact-checking my claims.
But you see I will label your comment as a troll and explain why I labelled as. Your comment would have been constructive if you demonstrated how my analysis was wrong and provided evidence that surpasses mine.
Indeed, you are using the common tactics of trolls and conspiracy lunatics: “You are biased in favour of mainstream narratives”. You see, this is where you have it wrong and this is how it is pointless to argument with you. I have it open to anyone to criticize my analysis but if you have a minimum expertise in scientific research, you cannot ignore the major flaws I have highlighted that makes this study flawed and its conclusions highly questionable. There is no “mainstream narrative”, there are just hard cold facts that just simply does not align to your narrative.
I will let your comment online so everyone can make a judgement, but I will likely not answer to your reply because I don’t think I can bring conspiracy theorists into reason.
LikeLike
Simon, I don’t trust you! 😉
Agreeing with “mainstream narratives” doesn’t mean someone is biased. I think you may be biased, because you don’t accept overwhelming evidence about the safety of vaccines.
If you don’t trust the “mainstream narrative,” what do you trust? Or do you simply have no option on this subject?
And one more question, please: what evidence would it take to convince you that vaccines are safe? It’s a somewhat rhetorical question, because I don’t think any evidence presented to you would suffice. If so, anything you have to say is meaningless.
LikeLiked by 1 person
What is mainstream- its the quantity of scientific papers publishred. If one has a different opinion, he/she should publish (very) sound scientific data to show, that mainstream is wrong. But only a mistrust without data is trolling around.
Also please present data and published papers, which show that the manifold of mainstream data are falsihied, or bad science or whatever.
Otherwise you are a real troll. One of many unscientific trolls in the antivaccine field.
LikeLiked by 1 person
What’s all this Public Relations nonsense that Pr. Exley is anti-vaccine? Why is there no criticism of Merck on this page? Merck refuses to give Exley the vaccine adjuvant used in Gardasil. What do Merck have against peer review? If Merck’s own studies cannot be repeated why don’t you criticize that?
It has long been know that the CDC has all the metadata it needs to run a vaxxed versus unvaxxed study on the US population. All these arguments about new studies being unethical is irrelevant. It is unethical that the CDC do not run the test on their database. As a pro-vaccine person myself i ask these questions. I want safe vaccines. The US Supreme Court gives vaccines the curious legal status of being “Unavoidable unsafe”. Let’s change that.
J.B. Hadley kicks off about the history of diseases, Measles and Pertussis. All pro-vaxxers I’ve come across know nothing about these statistics, the best comment I read was that statistics show further declines after vaccines were introduced. That’s great. But there is a hole in that due to diseases getting reclassified after the vaccine strain is distributed. The pro-vaccine camp is dominated by people that either don’t know the history or hide it. It’s very frustrating when only vaccine critics bring up these very valid points. It looks like us Pro-vaxxers don’t know what we are talking about. I blame the main stream media for not talking about these issues often enough.
Vaccine safety is not holding up from a risk / benefit point of view. We need the CDC’s research to reduce the risks by identifying health outcomes associated with vaccines. Let’s get every possible study done from existing CDC data, even studies that compare siblings from the same family where only one child is vaccinated. If the CDC has a 1000 of those, that’s a good study.
It’s not conspiracy theory to point out that cancer causing viruses have been found in vaccines, we know they were there as SV40. Instead of calling people names like “Anti-vaccine and “conspiracy theorists” let’s clear all this up and develop safe vaccines. At least we can find out who can’t get vaccines due to vaccine injury susceptibility like organ recipients.
I’m guessing a lot of people don’t understand basic science and it’s labels like “Anti-vaxxer” that they respond to more than understanding the science.
LikeLike
“I’m guessing a lot of people don’t understand basic science”. You see, thats the problem buddy. You dont understand the basic science. You dont understand that in order to make a bold claim like Exley did in this paper, you first need proper controls (If I tell your blood pressure is 180/120 and I dont give you the normal values, you would not realize you are a walking timebomb ready to die from a brain hemorrhage), techniques with such huge variability (if your error bars is 2-3 times your mean not only statistics will mean nothing, but also your technique is not reliable) or even claiming to see cell types just by looking a lousy immunofluorescence technique (even a trained neuropathologist cannot identify a brain tumor with such a poor staining).
You know maybe, just maybe, you just join my lab and do some real research as I do for 15 years of my existence. Even for a summer and see how challenging real basic science is. Who knows, I can put on a pet project in assessing BBB transport of aluminum in vitro.
LikeLike
[…] autistic brains are smothered in aluminum. Hardly! This study has been discussed here and here and here and does not show any link between vaccines and autism. JB goes on to pronounce these eleven […]
LikeLike
I have a few basic questions.
1. If vaccines are as safe as claimed, why do you think manufacturers don’t need liability?
LikeLiked by 1 person
Hi Don,
Thank you for your message. Well, manufacturers are held liable via the VICP. Feels like your child has a genuine vaccine injury? You can easily file a lawsuit to the VICP via a lawyer and make your case.
Or you can go the classic way, but it will cost you more and less chance to settle on. For more info on the VICP.
https://www.hrsa.gov/vaccine-compensation/index.html
Just a friendly reminder, I expect 2. and further questions to be specific to the blog post or I will consider it you are just interested in trolling this page.
Thank you.
LikeLike